
November Week 4
Syncope
John Willis. Pediatrics in Review 2000;21;201DOI: 10.1542/pir.21-6-201
Case 1
Jo-Jo is an 11-year-old girl brought in by ambulance to the ED after ‘‘fainting’’ this
morning during math class. She describes feeling ‘‘dizzy’’ and ‘‘wobbly’’ when she
stood up from her desk to answer a question. Witnesses report Jo-Jo became pale
then collapsed into her chair, unconscious for 15 seconds. There was no abnormal
movement or trauma noted. She woke up spontaneously feeling ‘‘weak.’’ Jo-Jo was
late for the school bus this morning and missed breakfast. Emergency medical
services (EMS) report normal vital signs during transport and a point-of-care glucose
of 92 mg/dL. Vital signs and physical examination are normal.
1) What is the most likely cause of the syncope?
2) What test would be useful in the ED to help differentiate this type of syncope from another more ominous type?
3) What would be important to ask in the family history?
4) What is the most common cause of syncope in patients
5) What would you advise to this patient and the parents?
6) What is the mechanism of this type of syncope?
Case 2
Enrique is a 3-year-old boy brought in by his mother to the ED after an episode of ‘‘fainting’’ this afternoon. His mother states Enrique went into the bathroom to ‘‘pee pee.’’ Two minutes later she heard the toilet seat bang and found him on the floor unresponsive. She witnessed no abnormal movement but his eyes were deviated to the left. He woke up 2 minutes later but remained confused for another 15 minutes. She noted he had wet his pull-ups but showed no visible signs of trauma. Enrique had a febrile seizure at age 2 but is otherwise healthy. Review of systems is negative. Vital signs and physical examination are normal.AnECGis performedand interpreted as normal.
1. What is the most likely cause of the syncope in this case and why?
2. What would be involved in the workup in this case?
3. Why is the age important in determining the type of syncope?
Case 3
Prince is a 10-year-old boy brought in by ambulance to the ED after ‘‘fainting’’ this
afternoon during recess. He says he was putting on his jacket and then woke up on
the ground with a bleeding chin. Witnesses report Prince collapsed to the ground
and failed to protect his chin from striking the floor. He was unconscious for 30
seconds before awaking spontaneously. There was no abnormal movement noted.
His father states he has ‘‘fainted’’ twice this year but has never injured himself or
visited a physician. There is no family history of sudden cardiac death. EMS report
a point-of-care glucose of 90 mg/dL and normal vital signs during transport. Vital signs
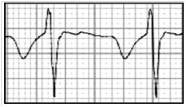
are normal. Physical examination reveals a 3-cm simple laceration to the chin. An ECG
is performed and the result is below.
1. What is the inciting factor here in the history clues you in this is cardiac syncope?
2. What is the cause of cardiac syncope in this case? What needs to be done in terms of evaluation/treatment?
3. What are the different causes of cardiac syncope
4. What is the type of arrhythmia that is precipitated by this disease that leads to syncope?
Case 4
J-Lo is a 14-month-old girl brought in by her grandmother to the ED after ‘‘fainting’’ this evening. Her grandmother states she became ‘‘very upset’’ when it was time to go to
bed and then collapsed into her crib. She was unconscious for 10 seconds before awaking spontaneously. She turned blue briefly but had no abnormal movements.
Her mother arrives and confirms this has happened one other time while being dropped off at daycare. The vital signs and physical examination are normal. An ECG is performed and interpreted as normal.
1. What is the most likely cause of syncope in this case?
2. What sort of education would you provide to the family?
3. Is treatment needed?